Rabies is an acute viral encephalomyelitis caused by members of the lyssavirus genus. The UK has been declared “Rabies-Free”. However, it is known that even in “Rabies-Free” counties the bat population posse a risk.
In the UK the only bat to carry rabies is the Daubenton’s Bat [Picture on the Left] and this is not a common bat in the UK. The UK and Ireland are Classified as “low-risk” for bat exposure. Despite our “low-risk” status in 2002 a man died from rabies caught in the UK from bat exposure.
Although rabies is rare it is fatal so we must treat appropriately, Public Health England – Green book details this.
Risk Assessment
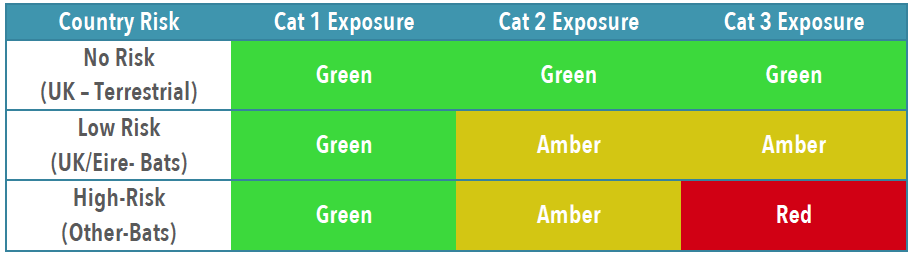
To establish patients risk and thus treatment you need to establish the Exposure Category and Country Risk [Link to Country Risk]
Exposure Category

Combined Country/Animal & Exposure Risk
Treatment
Obviously patients with wounds will need appropriate wound care and cleaning, specifics for rabies are below.
If in ANY doubt, or you feel you need advice about treatment contact: On-Call Microbiologist (who will contact PHE or Virology advice)

You will likely need to liaise with the duty pharmacist to obtain vaccine or HRIG – which may need to be sent from a different hospital. [it is probably worth trying to obtain the 1st weeks treatment if possible, to avoid treatment delays]
IN HOURS 08:30AM-5PM PLEASE CALL PHARMACY TO INFORM THEM TO EXPECT A DELIVERY OF IMMUNOGLOBULIN SO THIS CAN BE SEGREGATED FOR THE CORRECT PATIENT. PLEASE ASK TO SPEAK TO THE RESPONSIBLE PHARMACIST CRH (4218/4279) HRI (2422/7123)
Rabies and Immunoglobulin Service (RIgS), National Infection Service, Public Health England, Colindale (PHE Colindale Duty Doctor out of hours): 0208 327 6204 or 0208 200 4400




